0
Skip to Content
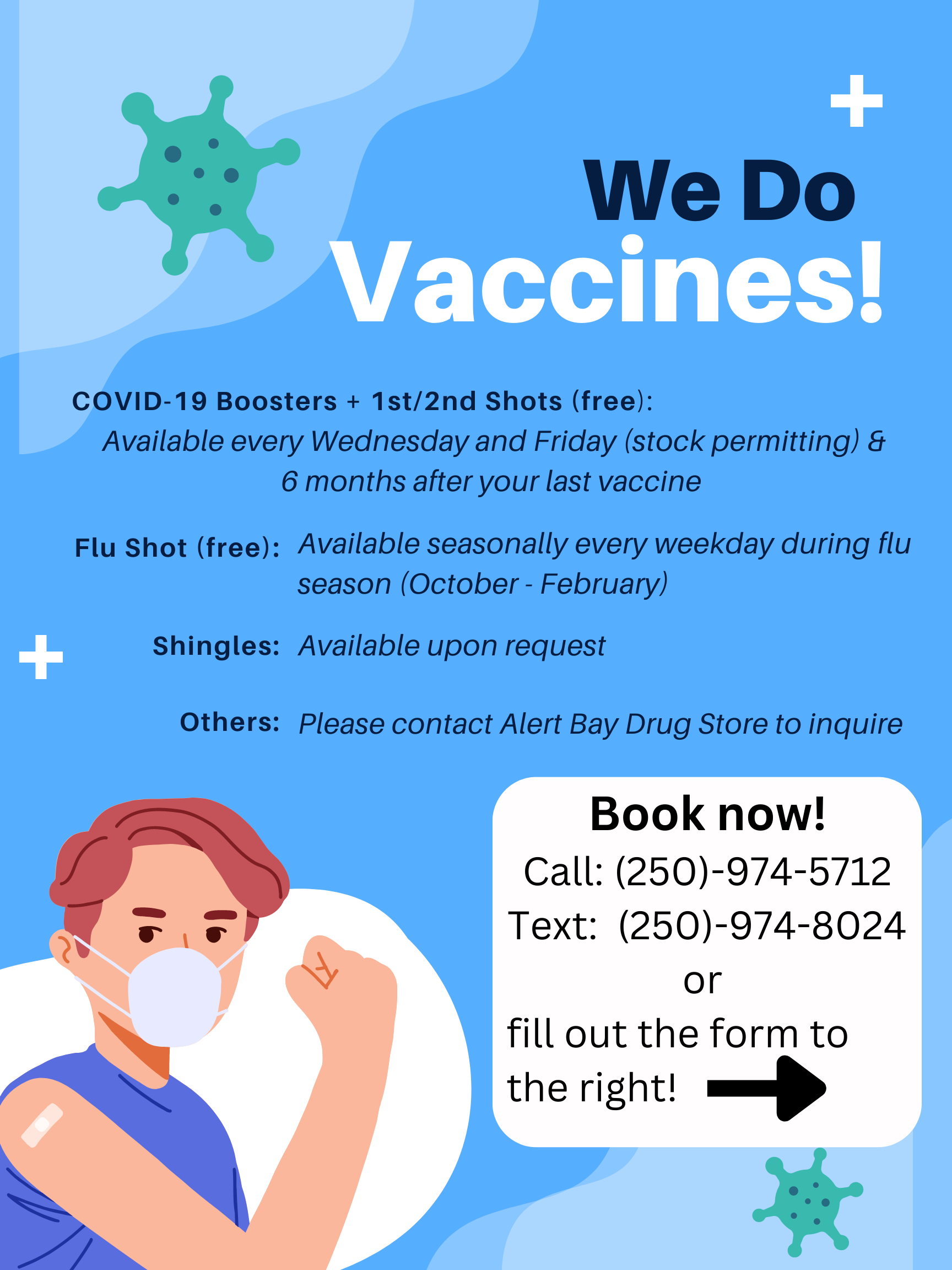
Alert Bay Drug Store - Est. 1949
Home
Order Here
Merchandise
Contact
Order Here
Open Menu
Close Menu
Alert Bay Drug Store - Est. 1949
Home
Order Here
Merchandise
Contact
Order Here
Open Menu
Close Menu
Home
Order Here
Merchandise
Contact
Order Here
Serving Alert Bay, Sointula, and surrounding communities since 1949
Here